
When you’re over 65, your body doesn’t just slow down-it rewrites how medicines work. Two organs, the liver and kidneys, become less efficient at processing and removing drugs. This isn’t just a minor detail. It’s why so many older adults end up in the hospital from medications that once worked fine. The truth? Drug metabolism changes in older adults aren’t theoretical. They’re measurable, predictable, and often overlooked.
What Happens to the Liver as We Age?
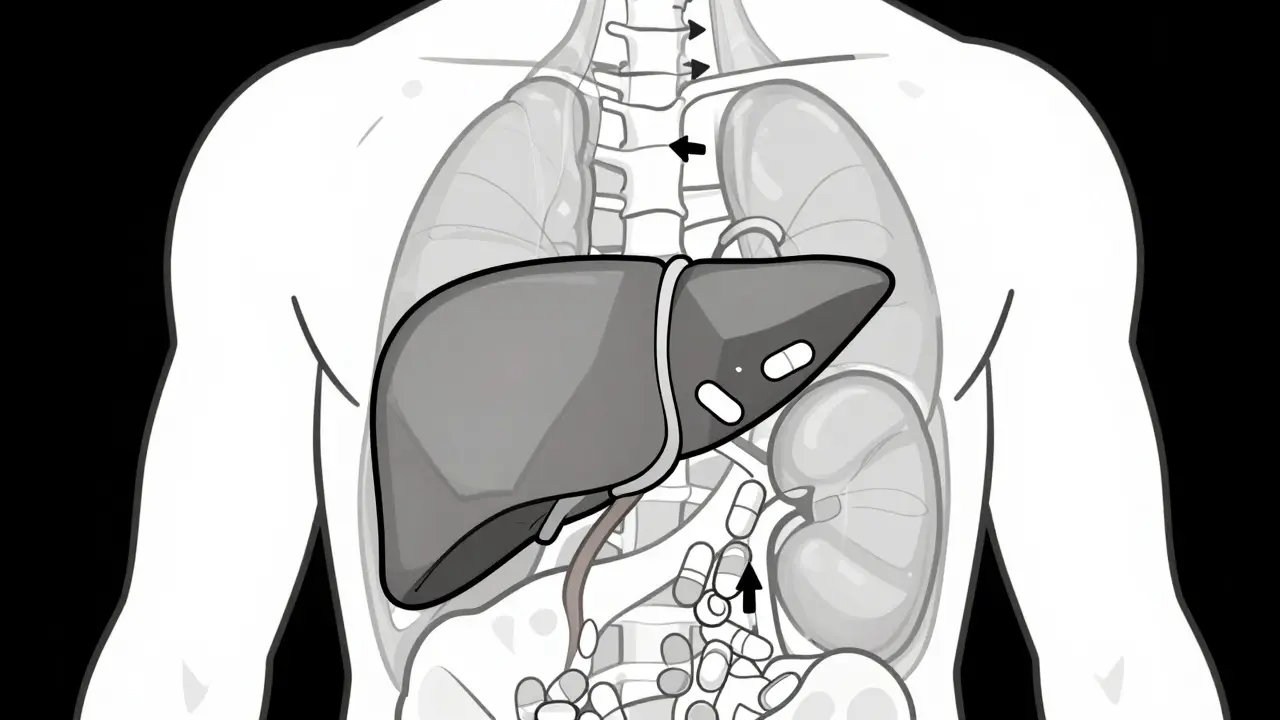
The liver doesn’t just get smaller with age-it gets slower. Studies show liver mass drops by about 30% between ages 30 and 80. Blood flow to the liver falls by 40%. That means drugs don’t get processed as quickly. For drugs that rely on liver flow-like propranolol, lidocaine, and morphine-clearance can drop by nearly half. These are called flow-limited drugs. If you take them at the same dose you did in your 40s, you’re likely getting too much.
But not all drugs behave the same. Drugs like diazepam, phenytoin, and theophylline are capacity-limited. Their metabolism depends more on enzyme activity than blood flow. Here, the story is different: enzyme levels stay fairly stable. Clearance drops only 10-15%. That’s why some older adults tolerate these meds better than others.
Then there’s first-pass metabolism. This is what happens when a drug is swallowed and absorbed through the gut before reaching the bloodstream. The liver normally breaks down a big chunk of it. But with reduced liver flow and mass, more of the drug slips through. That’s why drugs like propranolol and verapamil can have 25-50% higher bioavailability in older adults. A standard dose becomes a high dose. Dizziness, low blood pressure, even fainting can follow.
Kidneys Don’t Just Filter Less-They Stop Warning You
By age 80, kidney function typically drops 30-50% compared to when you were 30. This is measured by glomerular filtration rate, or GFR. But here’s the trap: serum creatinine-a common lab test-often stays normal. Why? Because older adults lose muscle mass. Less muscle means less creatinine is made. So your lab report says "normal," but your kidneys are working at 60% capacity. That’s why relying on creatinine alone is dangerous.
Drugs that leave the body through the kidneys-like digoxin, lithium, and many antibiotics-need lower doses. If you don’t adjust, they build up. Lithium levels can creep into toxic range. Vancomycin can damage kidneys if dosed by weight alone. A 2022 case study in the Journal of the American Geriatrics Society showed how adjusting vancomycin based on estimated GFR prevented kidney injury in a 78-year-old patient. Simple. Effective.
And here’s something newer: kidney problems can also mess with liver metabolism. Studies now show that when kidneys fail, certain liver enzymes (CYP450) slow down too. So even if a drug is cleared by the liver, poor kidney function can cause it to accumulate. It’s a hidden chain reaction.
Why Some Drugs Are Riskier Than Others
Not all medications are created equal in older adults. Some are ticking time bombs.
- Prodrugs like perindopril (an ACE inhibitor) need to be converted by the liver to work. With slower liver function, the active form forms too slowly. The patient gets no benefit-but still gets side effects.
- Drugs with narrow therapeutic windows like warfarin, digoxin, and amitriptyline leave little room for error. A small increase in blood level can cause bleeding, heart rhythm problems, or severe drowsiness. One Reddit user, "CaregiverInMA," described how their 82-year-old mother started on standard-dose amitriptyline for depression, then ended up in the ER with confusion and falls. Her liver couldn’t clear it.
- Over-the-counter painkillers like acetaminophen are a silent danger. The Acetaminophen Hepatotoxicity Registry shows it causes 50% of acute liver failure cases in people over 65. Why? Because the liver’s ability to detoxify it drops, and many older adults take it daily for arthritis without realizing the risk.
How Doctors Should Adjust Dosing (And Why They Often Don’t)
The American Geriatrics Society’s Beers Criteria® recommends starting doses 20-40% lower for drugs processed by the liver in patients over 65. For those over 75, reductions can be even higher. But here’s the gap: many doctors still prescribe by age alone, not function.
Two tools help fix this:
- Cockcroft-Gault equation: Estimates creatinine clearance. Still widely used, though outdated in some ways.
- CKD-EPI equation: Newer, more accurate. Doesn’t use race adjustments. Recommended since 2021.
Yet many clinics still use serum creatinine alone. That’s like trying to measure a leaky pipe by looking at the water pressure-not the actual flow.
Also, drug interactions get ignored. A patient on statins, blood pressure meds, and gabapentin might not realize these all compete for liver enzymes. The result? Toxic buildup. The START/STOPP criteria, updated in 2014-2015, help flag risky combinations. When used, they cut adverse events by 22%.
What’s Changing in 2026-and What’s Next
The FDA now requires drug trials to include older adults and analyze results by age. But only 38% of participants in new drug trials are over 65. That’s a massive blind spot.
Technology is catching up. In 2023, the FDA approved GeroDose v2.1, a software tool that simulates how a drug behaves in a specific patient based on age, liver enzymes, kidney function, and weight. No more guessing.
Research is also uncovering epigenetic clues. A 2023 study found 17 DNA methylation sites linked to CYP3A4 activity that change with age. This could lead to blood tests that predict how someone will metabolize drugs-not just their age, but their biology.
By 2030, experts predict personalized dosing algorithms could reduce adverse drug events in older adults by 35-50%. That’s not science fiction. It’s the next logical step.
What You Can Do Right Now
If you or a loved one is over 65 and on multiple medications:
- Ask your doctor: "Which of my drugs are processed by the liver or kidneys?" Get a clear answer.
- Request a GFR calculation using CKD-EPI-not just creatinine.
- Review all meds, including OTCs and supplements. Acetaminophen, ibuprofen, and herbal teas can all interact.
- Watch for new symptoms: dizziness, confusion, fatigue, nausea. These aren’t "just aging." They could be drug toxicity.
- Ask if a lower dose is possible. Many older adults take full adult doses out of habit.
Medicines save lives. But without understanding how aging changes the body’s chemistry, they can turn into hazards. The fix isn’t complex. It’s simple: treat the patient, not the age.










